
.webp)

Jessie is making lasagna when she notices her three-year-old, Milo, tucked in the corner of the family room. He’s watching Bluey, knees pulled to his chest, thumb resting comfortably between his lips. She calls his name. He smiles, thumb still there.
Jessie’s mother’s voice echoes in her head: “If he keeps doing that, his teeth will stick out like a bunny’s.” Is that true? Should Jessie start taping socks on his hands at night? Or will all this work itself out?
Thumb sucking is one of those childhood habits shrouded in half-remembered warnings and well-intentioned myths. As pediatric dental professionals, we talk parents through this crossroads (pun intended) every week. Below is the deep-dive we wish every family could read in a quiet moment—before the anxiety hits during dinner prep.


Why Kids Suck Their Thumbs in the First Place
Newborns rely on a “suck-swallow” reflex for survival. Long after bottle or breast feedings end, the reflex remains a built-in self-soother. Think of thumb sucking as nature’s pacifier: it lowers cortisol, regulates breathing, and helps toddlers drift to sleep. From a developmental standpoint, it’s completely normal up to age three.
Yet how a child sucks matters. Light, intermittent thumb resting exerts minimal force. Persistent, forceful sucking—especially if the thumb pulls forward against the upper front teeth—applies the same physics as certain orthodontic appliances, only in the wrong direction.
Quick answer: Occasional thumb sucking before age 3 rarely damages teeth. Continuous, forceful sucking that lasts beyond age 4 can tip upper incisors forward, narrow the palate, and create an open bite that often requires early orthodontic care.
The Dental Domino Effect: What Really Happens in the Mouth
- Pressure on the Roof of the Mouth
The palate (roof) is still soft cartilage in preschool years. Constant suction narrows its U-shape into a V, crowding future adult teeth. - Forward Tipping of Upper Front Teeth
Shear force on the backside of baby incisors flares them outward. When adult incisors erupt, they inherit that forward angle. - Open Bite Formation
The vertical gap you may see when a child bites down—front teeth not touching—isn’t just cosmetic. It can alter speech patterns and chewing efficiency. - Possible Speech Delays
Sounds such as “s,” “sh,” and “th” require precise tongue placement. A narrowed palate or open bite changes tongue posture, sometimes extending lisps into elementary school.
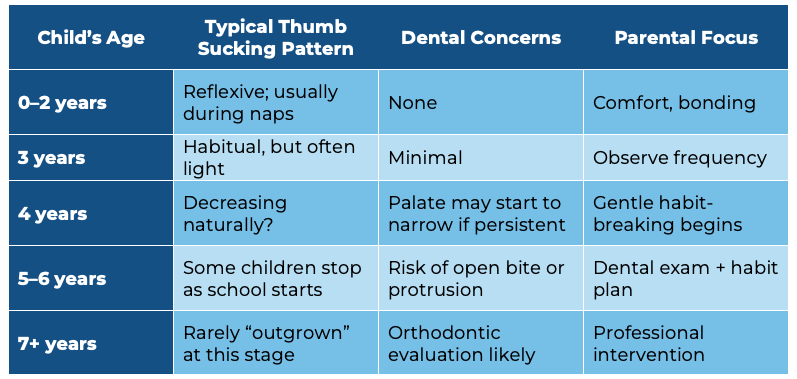
Milestones & Red Flags: A Year-by-Year Perspective
Gentle, Evidence-Based Strategies to Help Kids Quit
Important: Using harsh or negative methods can often have the opposite effect, pushing the habit to occur more secretly, especially during nighttime when thumb pressure tends to be strongest.
1. Turn Awareness into Ownership
Older preschoolers love being part of a “scientist experiment.” Have your child color-in a simple weekly calendar, marking thumb-free hours with stickers. The visual feedback converts an unconscious reflex into a conscious choice.
2. Swap the Sensory Need
Stress balls, textured blankets, or “hugging” stuffed animals give little hands something else to grasp at bedtime. For oral comfort, cold water sips or sugar-free popsicles can replicate the soothing mouthfeel without the prolonged pressure.
3. Celebrate Micro-Victories
Research shows that consistent, immediate praise—even for 15 thumb-free minutes—rewires habit loops faster than delayed, big rewards. Keep a jar of marbles: one marble per “win,” ice-cream date at 30 marbles.
4. Nighttime Reminders (Not Restraints)
A loose cotton mitten lightly taped at the wrist reminds kids during REM sleep without creating panic if they need bathroom breaks. It’s enough to wake subconscious awareness but humane compared to bitter nail polish or elbow splints.
5. When to Consider a Habit Appliance
If a child nears age six with an emerging open bite, a small intraoral crib device may be recommended. It’s painless, temporary, and works by blocking comfortable thumb placement. At our practice, we reserve this for cases where behavioral approaches have been tried consistently for at least three months.
Frequently Heard Parent Questions—With Candid Answers
- “Will the habit really disappear if we just wait?”
Most children do outgrow thumb sucking by school age, but about 15–20 percent do not. The later it lingers, the higher the orthodontic cost curve climbs. We encourage a “monitor until four, nudge by five” philosophy to keep options open and budgets friendlier. - “Pacifiers seem worse—so why not leave the thumb?”
Pacifiers come with an on/off switch (parents). You can limit them to bedtime or gradually clip the tip to reduce suction. The thumb, however, is available 24/7. Statistically, extended thumb suckers show slightly more dramatic palate changes than pacifier users, although both habits share similar risks. - “Could thumb-related open bite correct itself once he stops?”
Baby incisor flaring often self-corrects within six months after quitting. Palatal narrowing and skeletal open bites, however, usually do not. Early interception avoids possible jaw surgery later. - “My child sucks fingers instead of the thumb—same issue?”
Yes, though the force distribution differs. Index-finger sucking can push upper teeth forward and lower teeth inward, creating a scissor effect. The behavioral approach remains identical.
(More questions? We expand on these in our dedicated resource, Thumb Sucking and Your Child’s Teeth.)

A Moment in the Treatment Room
One afternoon, six-year-old Ari walks into our Dallas office clutching his Spider-Man plush. His front baby teeth flare forward like tiny wings, and an open bite lets you spy his tongue when he giggles. Dr. Tyler Driggers kneels to eye level, asks Ari to roar like a T-rex, and notes the bite gap.
Instead of lecturing, Dr. Driggers invites Ari to become a “Smile Hero.” They sketch a cartoon villain—“Dr. Thumb”—and map an escape plan: superhero pajama gloves, a sticker mission log, and a weekly FaceTime check-in with grandparents cheering him on. Seven weeks later, Ari’s nightly thumb need falls to zero. Re-evaluation at three months shows the open bite has cut in half, and speech clarity soars. The point? Success lives at the intersection of clinical timing and emotionally intelligent coaching.
The Pediatric Dentist’s Checklist (For Parents’ Eyes Only)
This is the closest we’ll come to a list—because sometimes tactical clarity trumps prose.
- Age 3: Mention habit at regular check-up; capture baseline photos.
- Age 4: Track frequency. Introduce gentle reminders if sucking persists more than eight hours/day.
- Age 5: Evaluate bite with a pediatric dentist. Start behavioral program if habit remains.
- Age 6: Consider radiographs and referral for habit appliance if orthodontic movement evident.
- Age 7+: Coordinate with orthodontist for palatal expansion or braces as needed.
(Need a baseline visit? Use our simple Appointment Request form.)
What We Tell Families in Dallas
At CrossRoads Pediatric Dentistry in Dallas, GA, thumb sucking isn’t an emergency—it’s a window of influence. Every month earlier that your child quits can save months in braces later. We advocate for a calm, collaborative approach: parent coaching first, small dental “training wheels” only if biology demands.
FAQ Section
Q1: At what exact age should I start worrying about dental changes from thumb sucking?
A: Biologically, palatal narrowing can begin as early as age four in heavy suckers. That doesn’t mean panic on the fourth birthday, but it does signal time to watch more closely. At our practice, we photograph the bite at routine cleanings; subtle shifts guide our coaching timeline and reassure parents when nothing has changed.
Q2: Do genetics play a role, or is thumb pressure the only culprit?
A: Genetics determine jaw size and tooth eruption angles. Habit pressure layers on top of that blueprint. A child genetically predisposed to crowding may develop noticeable misalignment faster under thumb pressure. Conversely, a genetically wide palate may tolerate longer thumb sucking without visible change—but the risk still exists.
Q3: Will my child need speech therapy if thumb sucking has caused a lisp?
A: Often, stopping the habit allows tongue posture to normalize, and mild lisps resolve on their own within months. If the open bite persists or if the lisp proves resistant, coordinated care with a speech-language pathologist accelerates progress. We refer proactively when articulation hasn’t improved three months post-habit.
Q4: Are bitter nail polishes safe for young kids?
A: Most commercial formulas use denatonium benzoate, the same agent in household cleaners to deter swallowing. While non-toxic in small doses, it can irritate sensitive skin and may transfer to eyes. We view these polishes as last-line adjuncts—effective for older kids motivated to quit but not for toddlers who explore with hands.
Q5: How long does a habit appliance stay in the mouth, and is it painful?
A: Crib or rake appliances typically remain for four to six months—long enough for the neuromuscular pattern to break. Installation is painless; mild tongue soreness fades within days. Kids adapt quickly, especially when they’re part of the decision. Proper brushing (we demo this in our Early Dental Care guide) prevents plaque buildup around the wires.
Bringing It All Together
Thumb sucking illustrates a broader truth in pediatric dentistry: small, everyday behaviors nudge growth plates and tooth buds more powerfully than most parents realize. Waiting isn’t wrong—but waiting without watching can shrink the window for simple, gentle solutions.
If you’re staring at your child’s cozy thumb tonight and feeling the swirl of “should I intervene?” remember Jessie and Milo. There’s a compassionate pathway from reflex to release. And you don’t have to walk it alone.
Ready for Personalized Guidance?
We’re happy to coach you through sticker charts, mitten tricks, or—if timing calls for it—habit appliances. Call 770-738-5437 or drop us a note through our Contact Us page. Your child’s future smile (and speech, and sleep) will thank you.




